
By Bridget K. Burke
If you are a nurse, or thinking about going into nursing, you may be hearing two very different messages about its future.
One message is that the future of nursing is bright. Americans are aging, chronic disease is rising, and patients will need care. Based on past patterns, the U.S. Bureau of Labor Statistics projects registered nurse employment to grow 5% from 2024 to 2034, with about 189,100 RN openings each year. Healthcare occupations overall are projected to generate about 1.9 million openings per year, largely from growth and replacement needs. (BLS)
The other message is that artificial intelligence is beginning to reshape medical work itself. Documentation, scheduling, triage, patient messaging, remote monitoring, discharge planning, clinical summarization, and logistics are all being redesigned. McKinsey reported in April 2026 that half of surveyed U.S. healthcare organizations were implementing generative AI, with attention shifting toward integration, return on investment, and agentic AI. (McKinsey, 2026)
So which message is right?
Both.
That is the nursing paradox.
Nursing is strong because America needs more care than the system can comfortably deliver. But nursing is vulnerable because the same pressures that make nurses essential — shortages, burnout, cost pressure, and complexity — are pushing healthcare organizations to automate more of the work around them.
- Nurse Practitioners (NPs): Approximately 235,000 to 355,000,
- Registered Nurses (RNs): Approximately 3.4 to 4.7 million actively licensed, making it the largest healthcare profession.
- Licensed Practical/Vocational Nurses (LPNs/LVNs): Around 641,000 to 973,788 licensed professionals.
At the top are advanced, specialized, and expert nurses: clinicians who manage complexity, interpret ambiguity, communicate risk, and carry responsibility for high-stakes decisions. These nurses may become more valuable with AI because the technology can extend their reach, sharpen their information, and reduce some administrative burden.
At the base are care-support roles: nursing assistants, aides, orderlies, and other workers who do much of the physical, hands-on, dignity-preserving work of care. These roles are not “safe” from automation forever, but they may be harder to replace quickly because bodies, rooms, mobility, falls, bathing, feeding, and comfort are difficult to automate reliably and affordably.
The most vulnerable layer may be the middle where the majority of nurses work, the registered nurses: routine, repetitive, protocol-driven nursing work where early- and mid-career nurses learn through exposure. That work may be easier to centralize, automate, monitor, or redesign through AI, virtual nursing, remote monitoring, and workflow tools.
That is the hollowing-out risk: AI may protect the top of nursing while weakening the middle layer that trains nurses to get there.
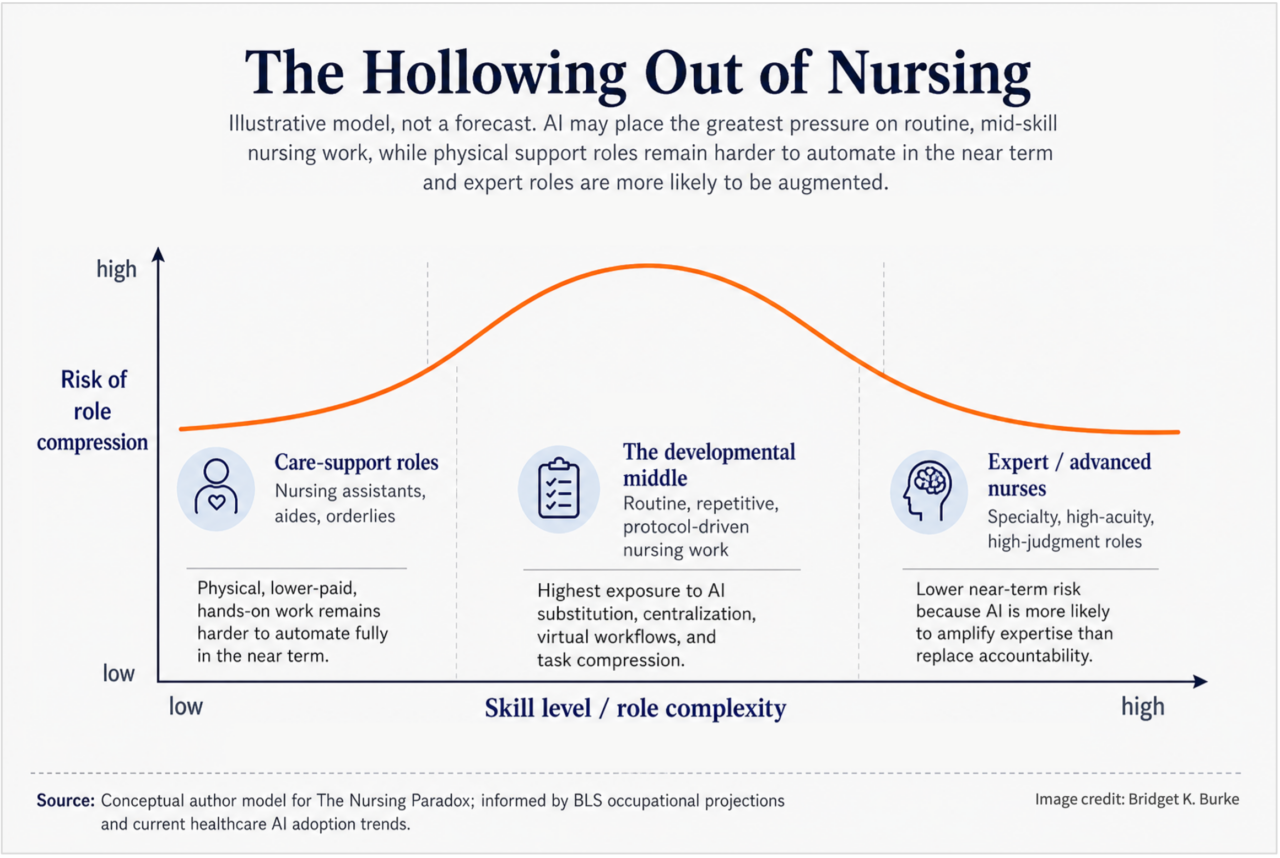
Figure 1. The hollowing-out risk: AI may not affect nursing evenly. The most exposed layer may be the developmental middle, where routine work helps nurses become experts.
The danger is not that AI simply “replaces nurses.” That is too blunt. The deeper danger is this: AI may strengthen expert nursing in the short term while weakening the pathway that creates expert nurses in the long term.
AI will not replace “the nurse.” It will unbundle nursing.
A nurse is not one task. A nurse is assessment, communication, judgment, documentation, physical care, medication administration, education, coordination, emotional presence, escalation, and pattern recognition, often all in the same hour. Some of that work is very hard to automate.
A frightened family does not need only an answer. They need a human being who can read the room. A patient who says, “I just don’t feel right,” may need someone who has seen that look before. A subtle change in breathing, mood, skin color, confusion, or silence may matter before the data catches up.
But other parts of nursing are much easier to automate, centralize, route, or support with AI.
Ambient documentation can reduce charting burden. The American Hospital Association highlighted real-world ambient AI deployments, including one nurse who reported that AI saved about two hours of charting during a 12-hour shift. (AHA)
That sounds like good news.
And in many ways, it is.
But every minute saved raises a question: who gets the minute?
Does the nurse get more time with patients? More time to think? More time to teach, mentor, recover, and notice?
Or does the organization capture the time as throughput?
More patients. More discharges. More messages. More alerts. More work packed into the same shift.
That is where the future gets complicated.

Figure 2. The impact of AI depends not only on time saved, but on where that time goes.
The first change may feel like relief.
In the near term, AI will probably not cause a sudden collapse in nursing jobs. The workforce is too large. The demand is too real. The work is too physical, regulated, relational, and unpredictable.
Instead, the first change will likely be compression.
The charting gets easier, but the shift gets faster. The handoff gets cleaner, but the assignment gets heavier. The dashboard gets smarter, but the nurse becomes responsible for watching more streams of information at once.
Imagine Maria, a med-surg RN in 2027.
When she logs in, AI has already summarized the overnight notes. A risk model flags two patients. A virtual nurse helps with discharge teaching. A robot delivers supplies. Her documentation is partly drafted as she speaks.
On paper, this is progress.
And it is.
Maria spends less time typing. She catches some issues earlier. She wastes fewer steps.
But by late afternoon, she feels the part the dashboard does not show. Her patient load has not dropped. The saved time has been absorbed into more throughput. She is doing less clerical work, but more exception management. Less typing, but more watching. Less searching, but more reacting.
This is not replacement.
It is recompression.
The top may benefit.
The bottom may linger.
The middle may be squeezed.
The future of nursing will probably not be evenly distributed.
At the top, advanced and highly specialized nurses may become more valuable. Nurse practitioners, nurse anesthetists, and nurse midwives are projected by BLS to grow 35% from 2024 to 2034, much faster than average. These roles involve diagnosis, treatment planning, complex management, accountability, and high-trust decision-making — the kinds of work AI may support but not easily own. (BLS)
At the support level, many roles may remain necessary longer than technologists expect. Patients still need to be moved, bathed, fed, turned, protected from falls, comforted, and watched. Bodies are not spreadsheets. Rooms are not chat windows. Human care is physical.
The most fragile layer may be the middle.
By “middle,” I do not mean one formal license category. I mean the developmental middle of nursing: early- and mid-career RNs, LPN/LVN roles, generalist bedside work, routine clinical environments, and the repeated everyday tasks where nurses build judgment over time.
That is where the real risk sits.
Not because all mid-career nurses disappear in five years. That is too extreme. The more realistic risk is that this layer becomes thinner, faster, more monitored, more centralized, and less educational.
And that matters because the middle is where expertise is made.
Routine is not just routine. It is practice.
This is the part healthcare leaders need to think about very carefully.
AI is excellent at absorbing routine. That is its promise.
But routine is also how people learn.
A new nurse does not become an expert by reading perfect summaries. She becomes an expert by seeing the same pattern many times, then recognizing the one patient who does not fit the pattern.
She learns from the admission that seems simple but is not. The discharge that becomes a family crisis. The patient who says the right words but looks wrong. The medication question that forces a pause. The handoff where something feels incomplete. The quiet room where the monitor looks fine, but the nurse’s gut says otherwise.
If AI removes too much of that ordinary exposure, it may leave humans with the extraordinary before they are ready.
That is the apprenticeship bottleneck.

Figure 3. The deeper risk is not only automation of tasks, but compression of the learning pathway that produces future expert nurses.
In the short run, AI may make expert nurses more powerful. They will supervise AI, catch its mistakes, interpret risk scores, and handle complex exceptions.
But eventually, if fewer nurses get the repetitions that build judgment, the profession may have fewer experts to replace the ones who retire.
And then the system may do something dangerous: default more high-level judgment to AI not because AI is truly better than expert nurses, but because there are not enough expert nurses left.
That is the real paradox.
AI may protect the top of nursing while quietly weakening the ladder that leads to it.
Put simply: if we use AI to advance nursing without protecting the learning ladder, we may strengthen today’s experts while making it harder to create tomorrow’s.
The old advice is no longer enough.
For decades, the career advice was simple: go into nursing. It is stable. It is meaningful. It is needed.
That advice is still partly true.
Nursing still offers purpose, mobility, human connection, and near-term opportunity. The National Council of State Boards of Nursing reported that more than 138,000 nurses left the workforce since 2022 and that almost 40% intend to leave by 2029, reinforcing concerns about ongoing labor shortages and systemic workforce challenges. (NCSBN)
But “go into nursing” is no longer specific enough.
The better advice is: Enter nursing strategically, not generically.
For career changers and recent graduates, the strongest paths will likely be the ones that move toward complexity, trust, and judgment.
That means high-acuity care. Specialty care. Advanced practice. Informatics. Quality and safety. Virtual care leadership. Complex care coordination. Oncology. Critical care. Behavioral health. Procedural settings. Home-based complex care. Roles where a nurse must communicate under uncertainty, notice what the system missed, and carry responsibility.
The weaker bet is assuming that routine, lower-autonomy, heavily protocolized work will remain untouched.
It may not disappear tomorrow. But it may become more compressed, more measured, more centralized, and less secure than the old nursing story suggests.
This is not destiny. It is design.
None of this means healthcare should reject AI.
That would be a mistake.
Nurses do not need more paperwork. They do not need more wasted steps. They do not need to spend their best human energy fighting bad software, hunting for supplies, or typing the same information three different ways.
AI can help.
But only if leaders ask better questions.
Not just: How many minutes did we save?
Also: Where did the minutes go?
Did AI give nurses more time with patients, or did it simply raise the speed limit? Did it reduce burnout, or hide burnout under better dashboards? Did it protect novice learning, or remove the very experiences that create judgment? Did it strengthen teams, or turn nurses into isolated supervisors of machines?
Responsible adoption will also require governance. The Joint Commission and the Coalition for Health AI released guidance in 2025 on responsible AI use in healthcare, including recommendations related to AI policies, local validation, monitoring, and integration into clinical and operational processes. (Joint Commission/CHAI)
That matters because healthcare AI is not just a technology purchase.
It is a workforce design choice.
The future of nursing will not look like the past.
The rearview-mirror model assumed that the future would be like the past, that nursing expertise moved up a ladder.
You started with basics. You repeated them. You made mistakes under supervision. You learned to prioritize. You learned what mattered. You learned when the protocol was enough and when it was not. Over time, you became the nurse everyone else trusted.
AI may change that ladder.
It may remove some bottom rungs. It may narrow the middle. It may make the top more technical, more specialized, and more dependent on human judgment over machine output.
That does not mean nursing has no future.
Nursing absolutely has a future.
But it may not be one future.
It may be two.
- One future belongs to nurses who can work with AI, question it, supervise it, and bring human judgment to complex care.
- The other future belongs to roles increasingly shaped by algorithms, virtual hubs, robotics, productivity metrics, and centralized workflows.
The difference between those futures will not be determined by AI alone. It will be determined by how healthcare leaders, educators, regulators, and nurses themselves choose to redesign the work.
The paradox
Nursing is necessary because America needs medical care.
Nursing is vulnerable because care is expensive, labor is scarce, and AI is arriving at exactly the moment healthcare organizations are desperate for relief.
- In the next few years, AI will likely reduce some burdens and intensify others.
- In five years, it will have reshaped staffing models.
But the deepest risk is not that AI replaces nurses.
The deepest risk is that AI replaces too much of the work that teaches nurses how to become proficient.
That is the nursing paradox.
The profession will remain indispensable but it will be reorganized by AI and its machines.
The question for a career changer is not, “Is nursing safe?”
The better question is, “What skill set will nurses have when AI dominates the profession?”
The charge to healthcare leadership is, “Do not abandon high-quality medical care for expedient short-term administrative gains.”
Bridget K. Burke is Principal Investigator at BridgetLab.ai. She serves on the CAHL Communications Committee, the HIMSS Global Professional Development Council, IEEE Robotics and Automation Society, and is the Editor-in-Chief of the IEEE AgeTech Quarterly Journal. She is a passionate advocate for making AI accessible, safe, and user-friendly for healthcare professionals. She enjoys exploring innovative technologies and sharing practical advice to help others navigate the evolving world of AI. Connect with Bridget on LinkedIn and direct message her your AI questions; she may answer them in a future article.
References
- U.S. Bureau of Labor Statistics. Registered Nurses, Occupational Outlook Handbook.
- U.S. Bureau of Labor Statistics. Nurse Anesthetists, Nurse Midwives, and Nurse Practitioners, Occupational Outlook Handbook.
- U.S. Bureau of Labor Statistics. Nursing Assistants and Orderlies, Occupational Outlook Handbook.
- McKinsey & Company. Generative AI in healthcare: Adoption matures as agentic AI emerges. April 2026.
- American Hospital Association. 6 health systems enhancing care delivery with ambient AI scribes. April 2026.
- National Council of State Boards of Nursing. Nursing workforce research and survey findings.
- The Joint Commission and Coalition for Health AI. Initial guidance to support responsible AI adoption. September 2025.